Best B2B Data Provider for Healthcare in 2026: Buyer's Guide
Choosing a B2B data provider for healthcare means balancing HIPAA-aware sourcing, NPI accuracy, and contact freshness. Here's how the major options compare in 2026 — and where to start.

Selling into hospitals, clinics, payers, or medtech buyers fails for one boring reason far more often than any pitch problem: the data is wrong. The decision-maker left 14 months ago, the email bounces, or the "verified" direct dial rings a closed department. A B2B data provider for healthcare has to clear a higher bar than a generic contact database, because the records are gated, the titles are dense with credentials, and the compliance surface is real.
This guide breaks down what actually separates healthcare-grade data vendors in 2026, how the major options compare, and how to pressure-test accuracy before you sign anything.
TL;DR#
- Healthcare data is a specialty, not a filter. Generic B2B databases under-cover providers, NPI numbers, and facility hierarchies — verify coverage against your exact ICP before buying.
- Accuracy beats volume. A 90%+ deliverable list of 5,000 right-fit contacts outperforms 50,000 stale records every time.
- Compliance is table stakes. Look for transparent sourcing, opt-out handling, and awareness of HIPAA boundaries (provider contact data is generally fine; patient data is not).
- The best stack is usually layered: a firmographic/provider database for targeting, plus a real-time finder/verifier like Tomba for fresh, deliverable contact details.
- Always run a sample test. Pull 100 records, verify them independently, and measure bounce rate before committing to annual pricing.
What is a B2B data provider for healthcare?#
A B2B data provider for healthcare is a vendor that supplies business contact and firmographic data specifically about healthcare organizations and the professionals inside them — think hospital procurement leads, clinic administrators, payer executives, pharmacy directors, and practicing providers identified by their NPI (National Provider Identifier).
Think of it like the difference between a general phone book and a specialist medical directory. A general directory lists everyone, but it won't tell you which cardiologist runs a 200-bed facility, what their group practice's tech stack looks like, or whether their direct email still works. Healthcare-specific providers enrich the standard firmographics (company size, revenue, location) with industry-specific attributes: bed count, specialty taxonomy, EHR system in use, affiliation networks, and provider credentials.
Technically, these vendors blend several sources — public registries (NPI, CMS), licensing boards, web crawling, opt-in panels, and contributory networks — then run data enrichment and verification to assemble a usable record. The quality gap between vendors comes down to how fresh those sources are and how aggressively they re-verify.

Why is healthcare data harder than generic B2B data?#
Four structural reasons make healthcare the hard mode of B2B data:
- Credential-dense titles. "Dr. Jane Smith, MD, FACC, Medical Director" is one person with four signals. Generic parsers mangle these, so seniority and specialty filtering breaks.
- High turnover and affiliation churn. Providers switch group practices, hospitals merge, and clinics rebrand constantly. A record that was perfect last quarter may now point at the wrong facility.
- Gated and fragmented sources. Much healthcare org data lives behind registries, licensing boards, and facility directories that don't expose clean APIs — so coverage varies wildly by vendor.
- Compliance boundaries. Provider business contact data is generally fair game, but anything touching patients invokes HIPAA. A serious vendor stays firmly on the business-contact side and documents its sourcing.
The practical takeaway: a database that looks impressive in a demo can collapse on your specific segment. Coverage of large IDNs (integrated delivery networks) tells you nothing about coverage of independent dermatology practices in the Midwest. Test your slice.
How do the main B2B data providers for healthcare compare?#
There's no single winner — vendors cluster into provider-intelligence platforms, broad B2B databases with healthcare coverage, and real-time finder/verifier tools. Most strong go-to-market teams combine two of the three.
| Provider type | Best for | Healthcare depth | Pricing model | Watch-out |
|---|---|---|---|---|
| Provider-intelligence platform (e.g. Definitive Healthcare) | Facility/IDN targeting, claims insight | Very high (beds, EHR, claims) | Enterprise annual | Expensive; contact freshness varies |
| Broad B2B database (e.g. |
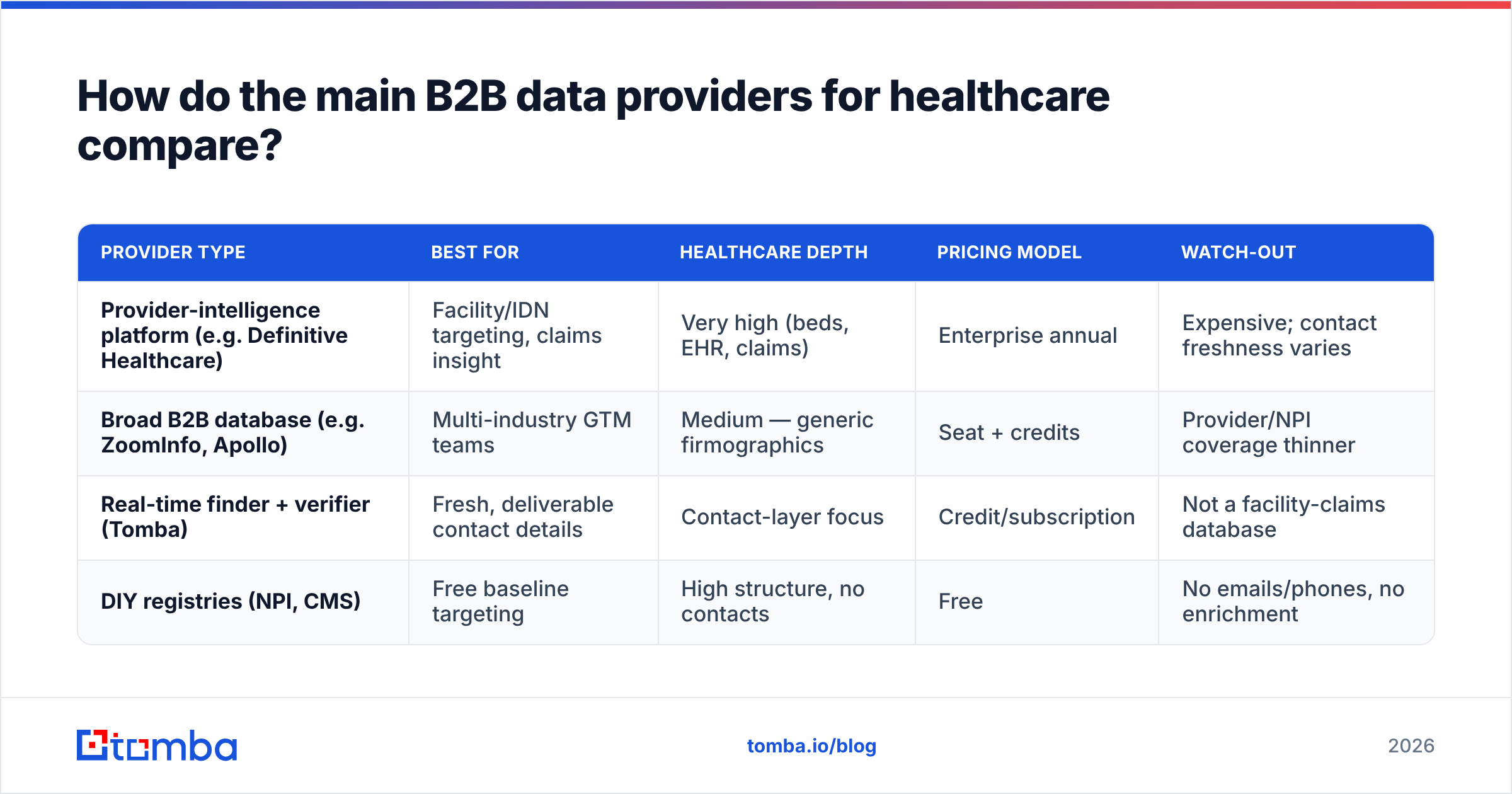
ZoomInfo, Apollo) | Multi-industry GTM teams | Medium — generic firmographics | Seat + credits | Provider/NPI coverage thinner | | Real-time finder + verifier (Tomba) | Fresh, deliverable contact details | Contact-layer focus | Credit/subscription | Not a facility-claims database | | DIY registries (NPI, CMS) | Free baseline targeting | High structure, no contacts | Free | No emails/phones, no enrichment |
A clean way to read this table: buy intelligence (who and where) from a provider platform or registry, and buy reachability (working email and phone) from a verification-first finder. Pairing the two beats overpaying one vendor to be mediocre at both.
For the reachability layer specifically, here's what to weigh:
- Accuracy guarantee: Does the vendor charge only for verified results, or for every lookup? Tomba's email verifier scores deliverability before you send, which directly cuts bounce rate.
- Source transparency: You should be able to see where a record came from. Tomba documents its data sources rather than treating provenance as a black box.
- Coverage of your segment: Run a sample. Volume claims are marketing; your hit rate on your ICP is the only number that matters.
- API and workflow fit: A great database you can't pipe into your CRM is shelfware. Check for a real email finder API, native integrations, and bulk processing.
What should you look for in a healthcare data vendor?#
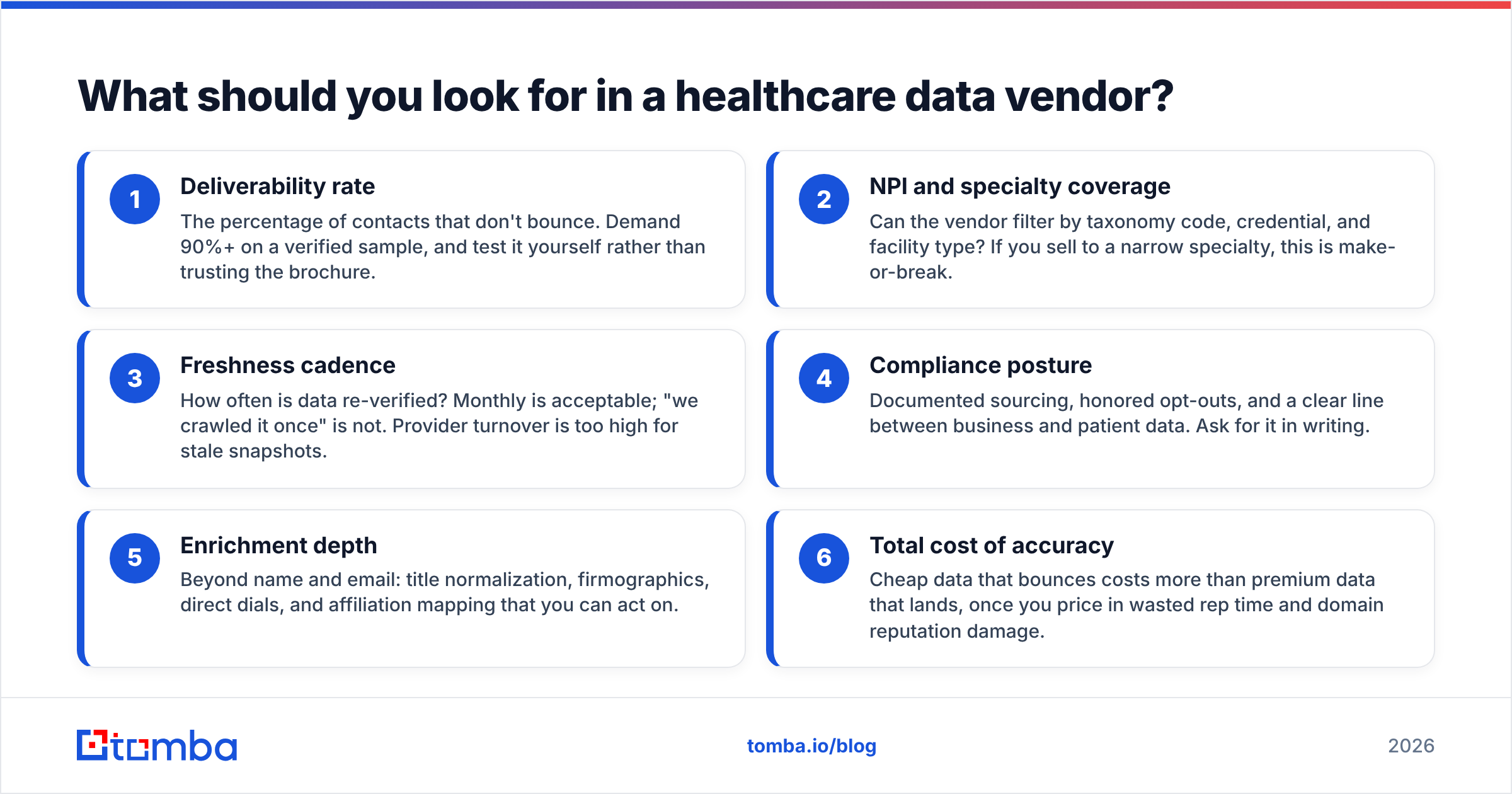
Score every candidate on six concrete dimensions instead of vibes:
- Deliverability rate — The percentage of contacts that don't bounce. Demand 90%+ on a verified sample, and test it yourself rather than trusting the brochure.
- NPI and specialty coverage — Can the vendor filter by taxonomy code, credential, and facility type? If you sell to a narrow specialty, this is make-or-break.
- Freshness cadence — How often is data re-verified? Monthly is acceptable; "we crawled it once" is not. Provider turnover is too high for stale snapshots.
- Compliance posture — Documented sourcing, honored opt-outs, and a clear line between business and patient data. Ask for it in writing.
- Enrichment depth — Beyond name and email: title normalization, firmographics, direct dials, and affiliation mapping that you can act on.
- Total cost of accuracy — Cheap data that bounces costs more than premium data that lands, once you price in wasted rep time and domain reputation damage.

That last point deserves emphasis. Bouncing into healthcare inboxes doesn't just waste a send — it erodes your sender reputation, which quietly tanks deliverability for every future campaign. The cheapest list is rarely the cheapest outcome.
How do you test data quality before buying?#
Run a structured 100-record bake-off. This is the single highest-leverage thing you can do, and most buyers skip it.
The test protocol:
- Pull a representative sample. Ask each vendor for 100 records matching your exact ICP — not their best-covered segment, yours.
- Verify independently. Run every email through a neutral email verification tool. Don't let the vendor grade its own homework.
- Spot-check 20 by hand. Confirm the person still holds the title at the listed facility via LinkedIn or the facility site.
- Measure four numbers: valid-email rate, catch-all rate, title-accuracy rate, and phone-connect rate.
- Price per usable record, not per record. Divide total cost by the count that actually passed.
A vendor selling 50,000 contacts at a 60% valid rate is selling you 30,000 usable records — and the wasted 40% still damages your domain. A vendor at 92% valid on a smaller pull is the better buy at the same headline price. For ongoing list hygiene, a bulk verify pass before each campaign keeps your numbers honest as data ages.
You can also sanity-check vendor reputation on independent review sites like G2 before you ever request a sample — patterns in recent reviews (especially complaints about staleness or support) tell you a lot.
Is a specialized provider better than a generic B2B database?#
It depends on how concentrated your healthcare focus is — but for most teams selling primarily into healthcare, a layered approach wins over any single generic database.
If healthcare is one of several verticals you sell into, a broad platform plus a strong contact-finder is usually enough. If healthcare is your whole business, invest in provider intelligence for targeting and pair it with a verification-first finder so your reach data stays fresh. The mistake to avoid is assuming a generic database's "healthcare filter" equals genuine provider coverage — it rarely does, and you'll find out only after the bounces roll in.
Here's the decision shortcut:
| Your situation | Recommended stack |
|---|---|
| Healthcare is 1 of many verticals | Broad database + Tomba finder/verifier |
| Healthcare-only, targeting facilities | Provider-intelligence platform + Tomba |
| Early-stage, budget-constrained | Free NPI registry + Tomba domain search |
| High-volume outbound | Tomba bulk finder + verification before every send |
Notice that the contact-and-verify layer is constant across every scenario. That's not an accident — targeting data tells you who to reach, but only fresh, verified contact data lets you actually reach them.
What does this cost in 2026?#
Pricing splits along the same lines as the vendor types. Enterprise provider-intelligence platforms run into five and six figures annually and are quoted, not listed. Broad B2B databases charge per seat plus credits. Verification-first finders price on volume and stay accessible to smaller teams.
For the contact-and-verify layer, Tomba's pricing is straightforward:
| Plan | Price | Best for |
|---|---|---|
| Free | $0 (25 searches/mo) | Testing accuracy on your ICP |
| Starter | $49/mo | Small teams, steady outbound |
| Growth | $99/mo | Scaling SDR motions |
| Pro | $249/mo | High-volume prospecting |
| Enterprise | Custom | API-heavy / large data ops |
Start on the free tier specifically to run the 100-record bake-off above. There's no faster way to learn whether a vendor's accuracy survives contact with your actual target list — and it costs you nothing but an afternoon.

How should you structure your healthcare data stack?#
Keep it to three layers and resist the urge to over-buy:
- Targeting layer — A provider-intelligence platform or the free NPI/CMS registries to define who fits (specialty, facility, size).
- Contact layer — A finder/verifier to attach fresh, deliverable emails and phones to those targets, and to re-verify on a cadence.
- Activation layer — Your CRM and outreach tooling, fed by clean data through native integrations so nothing rots in a spreadsheet.
The failure mode is collapsing all three into one over-priced vendor that's excellent at one layer and weak at the others. Buy best-of-breed per layer, connect them, and re-verify often. Healthcare data decays faster than almost any other vertical — your process for keeping it fresh matters more than which logo you started with.
The bottom line#
The best B2B data provider for healthcare in 2026 isn't a single product — it's a layered stack where targeting data and contact data each come from a vendor that's genuinely good at that job. Pick provider intelligence for who and where, and pick a verification-first finder for reachable and fresh. Then prove it with a 100-record test before you sign anything.
For the contact-and-verify layer — the part that decides whether your outreach actually lands — start with the Tomba Email Finder. Find and verify professional healthcare contacts by name, domain, or company, score deliverability before you send, and pipe clean records straight into your CRM. Spin up the free tier, run your bake-off, and let the bounce rate pick the winner.
Ready to find emails that actually work?
Join 150,000+ professionals who stopped guessing and started sending. Free credits on signup — no credit card required.
Get the Tomba newsletter
Practical outbound tactics and product updates — once every two weeks.
About the author