B2B Healthcare Marketing: The 2026 Playbook That Works
Selling into hospitals, payers, and health systems is a different game. Here's how B2B healthcare marketing actually generates qualified pipeline in 2026 — compliance, channels, data, and the metrics that matter.
TL;DR
- B2B healthcare marketing means selling to organizations — hospitals, payers, clinics, medtech buyers, pharma — not to patients, so the rules of consumer health ads barely apply.
- Sales cycles run 6–18 months across 5–10 stakeholders, so your strategy has to nurture committees, not capture leads.
- Compliance (HIPAA, FDA promotional rules, Sunshine Act) shapes what you can say and how you can target — bake it in from day one, not at legal review.
- Clean, verified contact data is the foundation: a wrong title or bounced email wastes weeks in a cycle this long.
- The teams that win in 2026 combine account-based outreach, clinical-grade content, and tight data hygiene — then measure pipeline, not vanity clicks.
What is B2B healthcare marketing?#
B2B healthcare marketing is how companies sell products and services to healthcare organizations rather than to patients. Your buyer is a hospital procurement lead, a health-system CIO, a practice administrator, a payer's VP of network strategy, or a clinical director — not the person in the waiting room.
Think of it like the difference between selling a car and selling a fleet. A consumer picks a car on a Saturday afternoon. A logistics company buys 200 vehicles after a procurement RFP, a finance review, a compliance check, and three rounds of stakeholder sign-off. Healthcare B2B is the fleet sale, except the fleet also has to satisfy a privacy regulator and a clinical safety board.
That changes everything about your go-to-market:
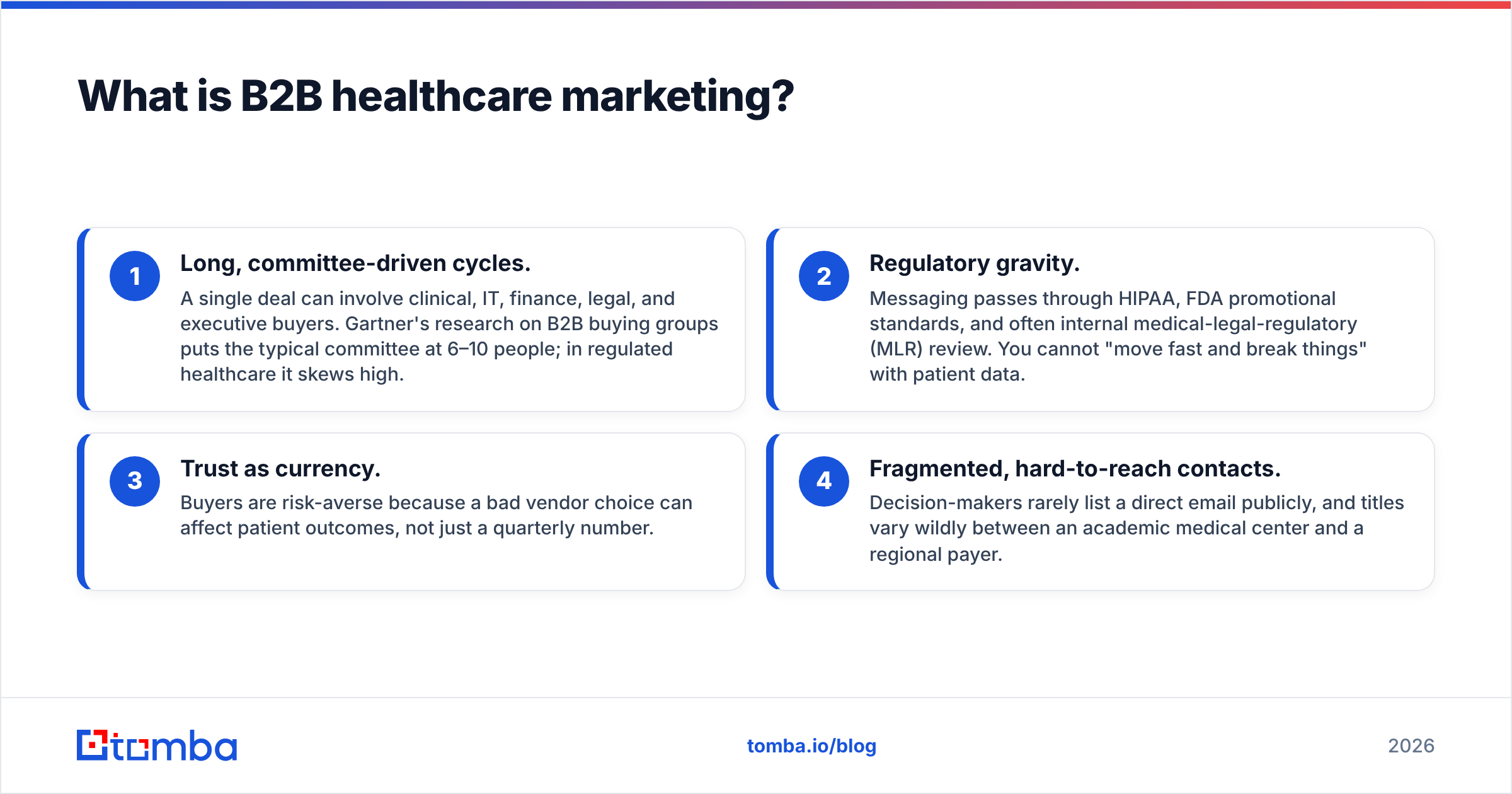
- Long, committee-driven cycles. A single deal can involve clinical, IT, finance, legal, and executive buyers. Gartner's research on B2B buying groups puts the typical committee at 6–10 people; in regulated healthcare it skews high.
- Regulatory gravity. Messaging passes through HIPAA, FDA promotional standards, and often internal medical-legal-regulatory (MLR) review. You cannot "move fast and break things" with patient data.
- Trust as currency. Buyers are risk-averse because a bad vendor choice can affect patient outcomes, not just a quarterly number.
- Fragmented, hard-to-reach contacts. Decision-makers rarely list a direct email publicly, and titles vary wildly between an academic medical center and a regional payer.
If you internalize one thing: you are not generating leads, you are warming an entire buying committee over quarters. Everything below serves that goal.
How is healthcare B2B marketing different from B2C health marketing?#
The two get conflated constantly, and it costs teams real money. Here's the clean split.
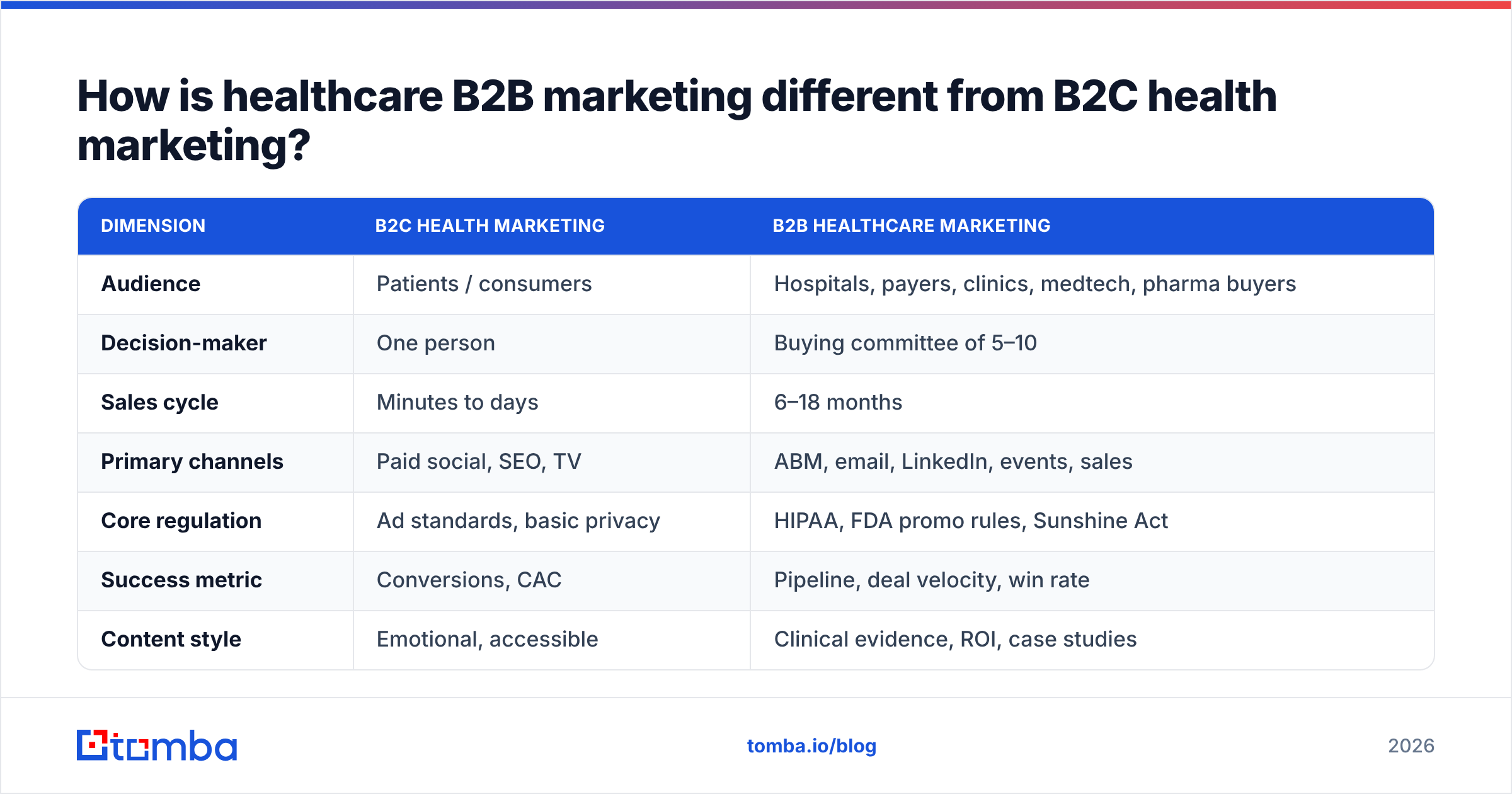
| Dimension | B2C health marketing | B2B healthcare marketing |
|---|---|---|
| Audience | Patients / consumers | Hospitals, payers, clinics, medtech, pharma buyers |
| Decision-maker | One person | Buying committee of 5–10 |
| Sales cycle | Minutes to days | 6–18 months |
| Primary channels | Paid social, SEO, TV | ABM, email, LinkedIn, events, sales |
| Core regulation | Ad standards, basic privacy | HIPAA, FDA promo rules, Sunshine Act |
| Success metric | Conversions, CAC | Pipeline, deal velocity, win rate |
| Content style | Emotional, accessible | Clinical evidence, ROI, case studies |
| Average deal size | Low | High (often six to seven figures) |
The strategic takeaway: B2C health marketing optimizes for volume and speed. B2B healthcare marketing optimizes for precision and patience. If your team is running a healthcare B2B motion with B2C dashboards — chasing cost-per-click and form fills — you are measuring the wrong thing and will kill long-cycle deals to hit a monthly number.
)
Which channels actually drive pipeline in 2026?#
No single channel carries a healthcare B2B program. The committee is too distributed. Here's where budget earns its keep, ranked by how directly each contributes to qualified pipeline.
- Account-based marketing (ABM). Pick the named accounts that fit your ICP — say, 200 IDNs or regional payers — and orchestrate coordinated touches across the whole committee. This is the backbone of modern healthcare B2B because it matches your effort to the committee reality.
- Targeted email outreach. Still the highest-ROI direct channel when your data is clean. A precise note to a named clinical director beats a thousand impressions. The catch is data quality — covered below.
- LinkedIn and social selling. Healthcare executives research vendors quietly on LinkedIn before they ever raise a hand. Consistent thought leadership plus direct LinkedIn outreach builds familiarity ahead of the buying window.
- Industry events and associations. HIMSS, regional HFMA chapters, payer summits — these compress relationship-building that would otherwise take months of cold touches.
- Evidence-based content and SEO. White papers, clinical outcome studies, ROI calculators, and webinars feed the long research phase. Buyers self-educate; give them the documents their procurement team will demand anyway.
- Webinars and peer panels. A panel of respected clinicians or CIOs does more to de-risk you than any ad creative.
Note what is not on this list: broad paid social aimed at "healthcare professionals," generic display, and off-the-shelf email-finder-vs-competitor charts. They burn budget without touching the committee.
)
How do you stay compliant without going invisible?#
Compliance is the part teams either over-fear (and freeze) or under-respect (and get fined). The honest answer: you can run aggressive, effective B2B healthcare marketing and stay clean, if you understand which rules touch which activity.
- HIPAA governs protected health information (PHI). In B2B, you are usually marketing to professionals about products, not handling patient records — so most outreach is outside HIPAA's core scope. The risk appears when your product touches PHI (EHR integrations, analytics) and during demos or data-sharing. Use Business Associate Agreements and never let real patient data into a marketing asset.
- FDA promotional rules apply if you market regulated devices or drugs. Claims must match the cleared/approved labeling. This is why medtech and pharma route everything through MLR review.
- The Sunshine Act (Open Payments) requires reporting certain transfers of value to physicians and teaching hospitals. Your "free dinner at the conference" can become a reportable event.
- CAN-SPAM and global privacy laws (GDPR for any EU contacts) still apply to your outbound email. Honor opt-outs, identify your sender, and keep suppression lists current.
The practical workflow: build a lightweight pre-approval path with legal/MLR for reusable message templates, so reps aren't waiting weeks per email. Approve the framework once, then let the team operate inside it.
For background on keeping outbound itself healthy and out of spam folders, our primer on email deliverability pairs well with the compliance basics above — deliverability and consent are two sides of the same "don't get blocked" coin.
Why is contact data the make-or-break factor?#
Because in an 18-month cycle, a single bad data point compounds. Email the wrong "Director of IT," and you don't just waste one send — you may burn the only warm intro you had into that account, then spend a quarter trying to recover.
Healthcare contact data decays faster than most industries. Clinicians change affiliations, hospitals merge into systems, and titles get reorganized constantly. Industry estimates put B2B data decay around 30% per year; in provider organizations the churn is often worse. A list you bought in January is materially wrong by summer.
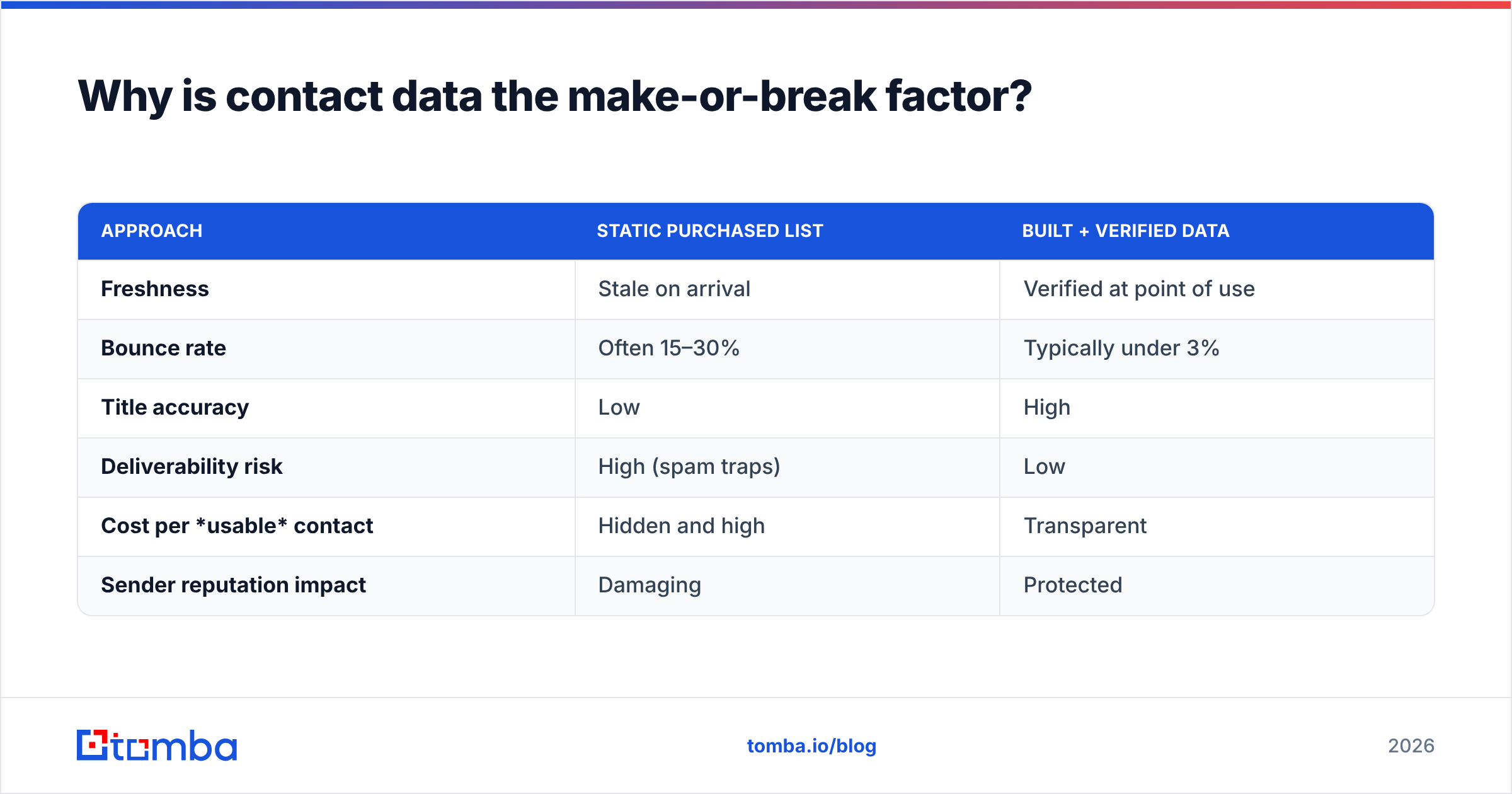
That's why mature teams stop buying static lists and start building and verifying their own from current sources. The difference looks like this:
| Approach | Static purchased list | Built + verified data |
|---|---|---|
| Freshness | Stale on arrival | Verified at point of use |
| Bounce rate | Often 15–30% | Typically under 3% |
| Title accuracy | Low | High |
| Deliverability risk | High (spam traps) | Low |
| Cost per usable contact | Hidden and high | Transparent |
| Sender reputation impact | Damaging | Protected |
A practical stack for sourcing committee contacts:
- Find the right people by company. Use domain search to pull the email patterns and named contacts at a target health system, then narrow to the roles on your buying committee.
- Find specific decision-makers. When you know the name and the org, an email finder gets you the professional address without guessing formats.
- Verify before you send. Run every address through an email verifier so bounces never touch your sending domain — critical when deliverability protects a multi-quarter relationship.
- Enrich for context. Layer firmographic and role data with data enrichment so reps personalize to the buyer's actual mandate (cost reduction, interoperability, quality scores) instead of sending generic pitches.
Get this layer right and every downstream channel performs better. Get it wrong and your best creative dies on impact.
What metrics prove your B2B healthcare marketing is working?#
Drop the B2C dashboard. Long, committee-driven cycles need leading and lagging indicators that respect the timeline.
- Pipeline created (and influenced). The number that matters: dollars of qualified pipeline your marketing sourced or touched. Influence matters because committees are touched by many plays.
- Account engagement depth. In ABM, track how many committee members at a target account are engaging — one champion is fragile, four is a deal.
- Sales cycle velocity. Are deals moving between stages faster than your baseline? Faster velocity is the clearest proof your content is de-risking the buyer.
- Marketing-qualified accounts (MQAs), not just leads. A single marketing qualified lead means little when you're selling to a group; account-level qualification is the honest unit.
- Win rate by segment. Track win rate by org type (academic medical center vs. community hospital vs. payer) to reallocate budget toward what closes.
- Data health. Bounce rate, contact verification rate, and list freshness. Boring, and the highest-leverage metric most teams ignore.
A reasonable 2026 benchmark hierarchy: optimize data health weekly, engagement and velocity monthly, pipeline and win rate quarterly. Report up on pipeline; manage internally on the leading indicators.
What does a 90-day healthcare B2B program look like?#
If you're standing up or fixing a program, here's a concrete sequence that respects compliance and the long cycle.
- Days 1–15 — Define the ICP and committee map. Name the account types and the 5–10 roles you must reach in each. Document the titles as they actually appear in provider vs. payer vs. medtech orgs.
- Days 15–30 — Build clean data. Source and verify committee contacts using the data stack above. Establish your bounce and verification baselines now so you can prove improvement later.
- Days 30–45 — Get message frameworks pre-approved. Run reusable templates through legal/MLR once. Build the SPF/DKIM and warmup foundation so deliverability is solid before volume ramps.
- Days 45–75 — Launch ABM + multichannel touches. Coordinate email, LinkedIn, and content across named accounts. Measure account engagement depth, not click counts.
- Days 75–90 — Read velocity and double down. Review which segments are advancing, reallocate budget, and feed sales the enriched context they need for the human conversations that close healthcare deals.
You can run the first two weeks of data work yourself with a Chrome extension and a bulk email finder for the named-account lists, then automate the refresh as accounts churn.
Common mistakes that quietly kill healthcare pipeline#
- Treating it like B2C. Chasing volume metrics and cheap clicks for a six-figure committee sale.
- Single-threading. Betting the deal on one champion who then changes jobs — a near-certainty in healthcare over an 18-month cycle.
- Buying stale lists. The fastest way to torch sender reputation and waste a quarter.
- Bolting on compliance late. Sending creative to MLR at the end instead of approving a framework up front.
- Generic messaging. A payer cares about network cost; an academic medical center cares about research and quality scores. Same email to both signals you don't understand them.
Avoid these five and you're already ahead of most competitors in the category.
The bottom line#
B2B healthcare marketing rewards precision and patience. You're warming a committee over quarters under real regulatory constraints, so your edge comes from clean data, compliant-by-design messaging, and metrics that measure pipeline instead of clicks. Nail the data layer first — it multiplies everything else.
When you're ready to build accurate, verified committee contacts for your target health systems and payers, start with the Tomba Email Finder. Pull the right decision-makers by name or domain, verify before you send, and protect the sender reputation that long healthcare cycles depend on. Check the Tomba pricing — there's a free tier with 25 searches a month to test it against your account list before you commit, with paid plans starting at $49/mo when you scale.
External references worth bookmarking: Gartner's B2B buying research, HubSpot's marketing benchmarks, and verified peer reviews on G2 when you vet any vendor — including us.
Ready to find emails that actually work?
Join 150,000+ professionals who stopped guessing and started sending. Free credits on signup — no credit card required.
Get the Tomba newsletter
Practical outbound tactics and product updates — once every two weeks.
About the author